


On prostate cancer

This post is aimed at male readers over 50 years of age (if this isn’t you, but you know someone that is, please pass it on). Please read it, and if you have not done so already, please act upon it. Your life may depend on it. Prostate cancer is the most common of male cancers. I have seen it stated that almost all males die with prostate cancer, that is to say, either with it, or of it. So this means you. Go to your doctor, or your hospital, and ask for a PSA test.

Back in 2017, living then in the UK, I had a shaking fit in bed one night. Feeling poorly in the morning I got a doctor to come around (they still did that, then). He told me I had a bladder infection and prescribed antibiotics. They did the job. A few weeks later I had a recurrence, same prescription. And a third time, a few weeks after that.
On the fourth occasion, I was in China. The following morning I went to the Shekou People’s Hospital in Shenzhen (they don’t do General Practice services in China) to beg some antibiotics, and went up to the window to register. This was at 9.30 am. At 10.10 am I was with a consultant urologist. Can you imagine that happening in the National Health Service (NHS) in Britain? He put me through a series of tests which took most of the morning and I went back to meet him at 2.00 pm. The results were all on his desk. He told me that there was a fair chance that I had prostate cancer.
A week or two later I was back in the UK and I took this news to my General Practitioner who showed no sign of shame whatsoever. They were able to get me a hospital appointment quite quickly, the diagnosis was confirmed, and I was put on blocking medication (of which more below) until I could get treatment. I had to wait almost a year. I was put on a course of radiography, 20 daily exposures. This was 2018. The only side effect I had was anal bleeding which lasted for about three years. Fortunately it turned out that the cancer had not escaped to other parts of my body, and I owe that good fortune to the Chinese health system, not to the NHS, with whom alone I would probably have died by now, as the cancer would have spread, if not diagnosed in time. That is why you must catch it early, so get a test now.
The test for prostate cancer is the PSA and I then subsequently had to take a check every six months. The onset of concern is when the level rises above four. After three years, in January 2021 I was in China again, the test was due and I went to the University of Hong Kong Hospital in Shenzhen for the test. Alarmingly the result was twelve, it was rising quite quickly and treatment was urgently needed.
They put me straight away on the blocking course I mentioned above. Every three months I have a capsule injected into my belly, this contains goserilin which blocks the formation of testosterone, which is the agent which is responsible for the onset and growth of the cancer. There is also a daily tablet, bicalutamide. Every six months I take a blood test at the hospital which estimates PSA and testosterone content, both of which have remained virtually at zero. I have less testosterone than a woman, so one side effect I experience I will leave to your imagination.
Writing this article it occurred to me that it was not clear what the bicalutamide tablet is for, and so I did a search for it. I found two statements, one said it is for cases where the cancer has spread into the body, which does not apply to me, and the other says it should be taken for at least two years after the start of the implant treatment, and I have now scored up three and a half years. I have always been wary of taking unnecessary medication: I stopped taking statins some time ago, though I take amlodipine 10 mg for blood pressure which seems to do the job. There is a list of possible side effects some of which I experience, so I decided to stop today, September 4. I have a PSA due in one month’s time, so let’s see what transpires….

One month later I am feeling OK, possibly experiencing less of those side effects. I have a PSA due tomorrow….
OK, here’s the full report, on tests taken on October 4th, a month since I stopped taking the tablets. It was available for download that same evening.
Let’s focus on the bits that matter, the testosterone and the PSA.
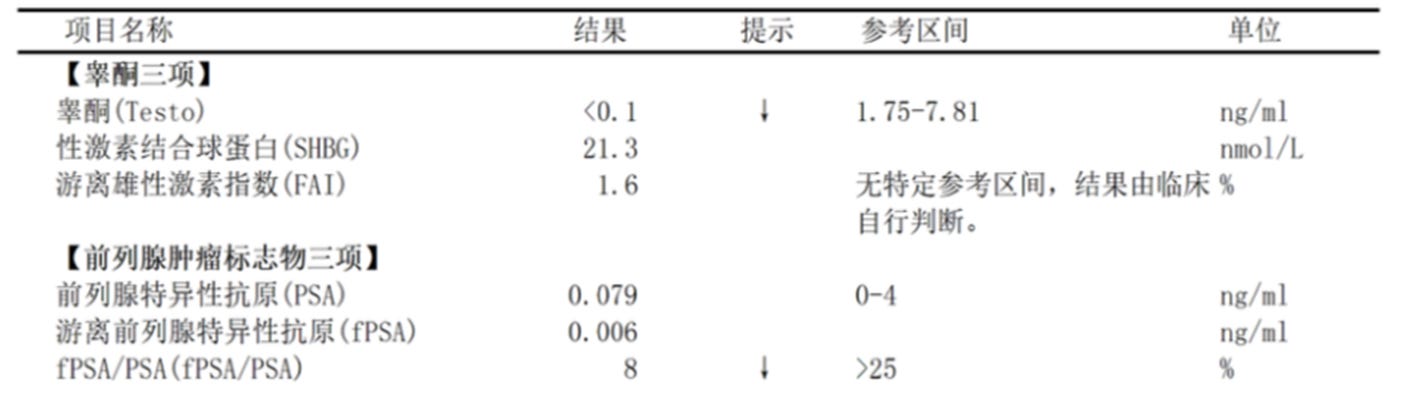
Testo(sterone) is less than 0.1, so that’s basically zero. Normal range for a male is 1.75 to 7.82 so no problem.
PSA is 0.079, normal is 0 to 4. Six months ago it was 0.089, so one month without bicalutamide has had no deleterious effect. I’ll stay off them: next test is January 4, 2025. If still alive, I’ll check back with you!
So don’t forget, if you are male and over 50. It could be a matter of life or death.
Yours.
……………………………………………………………………………………………………………………………………………………..
OTHER MATTERS
Auschwitz: six facts, and seven questions
I decided not to publicise this post on Moon of Alabama last week since, as I understand it, MoA is published in Germany, it is illegal to discuss such matters there, and thus it might put the host Bernhard in a difficult position.
It is not illegal in the UK, but nevertheless I have been banned by the Craig Murray blog for trying to publicise it there.
The Unz Report is just about the last such bastion of free speech that I am aware of, and I have had considerable responses from postings there. Unz (a Jew) has, on the side of an intellectual audience, a nasty white supremacist following, but at least it’s free speech there and very anti-Zionist apart from one head case, Ron takes a laid back attitude and he himself describes his website as “very lightly moderated”, so you take the rough with the smooth in the interests of free speech. Recommended, if you haven’t followed.
At the time of writing: Auschwitz: six facts, and seven questions has received 1,709 views in just one week. Anyway, you can still read it here:
https://open.substack.com/pub/waltking/p/auschwitz-six-facts-and-seven-questions
The Chinese Hakka minority
I received some queries in the comments asking about the Hakka minority.
I have compiled few clips from earlier films and added a commentary.
In the first, the woman on the boat is identifiable as a Hakka because of her distinctive hat.
Herewith, 9 minutes.
A Stranger in a Strange Land, episode one
This introduction to a series of nine about China has had a remarkable set of views considering that I gave it no publicity whatsoever. I shall post episode two next Wednesday, which is the sweep of history of contacts between western nations and China across about 2,000 years: “East Meets West”.
Meanwhile, if you haven’t seen it, you can find episode one here “China - Another Planet” - and visit Guangdong, Sichuan and Shaanxi provinces: 30 minutes.
https://rumble.com/v5hr45m-a-stranger-in-a-strange-land-episode-1.html
Stick with it to the end to see the most remarkable sight in China (perhaps in the world), the Terracotta Army.
This article is about cancer which is an anaerobic condition. In other words, it does not require oxygen. The organizations for which oxygen is a plosion live in heat vents in the ocean from underseas volcanoes or in places like Yellowstone park in the US.
The standard treatment of cancer is to target cancer cells. Alternative treatments based on the metabolic aspects have been around for decades but discouraged because of the influence of Big Pharma which sells cancer drugs that can cost $100,000 per year.
There are many alternative treatments inclusive integrative cancer treatment which is an adjunct to regular treatments using supplements. An internationally recognized MD has spent thousands of hours researching and consultation and produced a book that is downloadable for free.
Dr Marik was a founder of flccc.net - Front Line Critical Covid Care associates, an organization formed to treat covid with alternative methods during the "pandemic". The Cancer Care book is available on Amazon and can be downloaded here. There is a lot of organic chemistry involved in this book which has an overview and 1457 references.
https://covid19criticalcare.com/wp-content/uploads/2023/06/Cancer-Care-FLCCC-Dr-Paul-Marik-v2.pdf
"Integrative Oncology. Provision of care by a “true integrative oncologist” is the preferred
model of care for the patient with cancer. An integrative oncologist is dual qualified/certified
in orthodox medicine (oncology) as well as in integrative medicine (complementary
medicine). In many countries — including Israel, Germany, Switzerland, India, and other
countries in Asia — by default most oncologists are dually trained and function as
integrative oncologists. This is distinct from the United States, Australia, and some European
countries, where most oncologists follow the traditional orthodox approach.
The integrative oncologist has a diverse array of tools (therapeutic options) in his/her
toolbox and formulates an individualized and unique treatment plan for each patient. The
integrative physician and patient co-design an integrative treatment plan, recruiting the
“best of both worlds.” This may entail the use of chemotherapeutic agents/radiotherapy
together with complementary medicine or complementary medicine alone. Patients
participate in their treatment plans in a shared decision-making model. There is open
patient-physician communication that is non-judgmental and in keeping with the patient’s
cultural beliefs.
Integrative oncology involves a multidisciplinary team with caregivers committed to an
integrative care model. The major focus of care is the patient’s quality of life with an
emphasis on a) relief of symptoms, anxiety, and pain, b) quality of sleep, c) nutrition, d)
nutraceutical/herbs and repurposed drugs, and e) lifestyle changes. Integrative oncology
complements conventional medicine while keeping within the boundaries of scientific rigor.
Integrative medicine strives to be based on rigorous research, conducted in accordance with
scientific methodologies. Integrative oncology focuses on pragmatic research; pragmatic
trials test interventions in the full spectrum of everyday clinical settings, in order to maximize applicability and generalizability. Such pragmatic trials allow for a multimodal
integrative approach, are individualized, and with patient-centered outcomes. Patients in
countries where care is being managed by “orthodox” oncologists should consult with
integrative primary care physicians. "
Hi Walt,
Hope I find you well.
In my ongoing research on Pb I came across a particular supplement that seems to be gaining much interest in research circles, especially with regards to potential use as an antioxidant and anti-cancer treatment.
Berkley, UC, are heavily into the research and even have their own formulation available on mail-order.
It's called 3,3 diindolylmethane (DIM), and it is formed in small amounts in the body from brassica/cruciferaceae vegetables.
It seems linked to CB1 and CB2 cannabinoid receptors in the GI tract, and cannabidiol oil (CBD) itself has a growing body of evidence to support its use in prevention and spread of some cancer cell lines.
You can find some reasearch about it here:
https://pmc.ncbi.nlm.nih.gov/articles/PMC4197384/
and the Berkley page can be found here:
https://www.berkeleyformula.com/
Just thought it might arouse your interest.
All the best.
Jonathan